Forecast for 30 U.S. Cities The United States Environmental Protection Agency recently
began issuing a daily UV
FORECAST for 30 metropolitan areas around the country.
Non-Cancerous findings associated with radiation damage:
RadioDermatitis: Clinical Photos, chest, post mastectomy,(1)
, hand, occupational exposure, (2)
, cheek, post SCC (3)
, neck, post SCC, (4)
Advanced Photodamage in a Normal Host
Solar Elastosis EM
. This is a disease of dermal sun damage which is irreversible.
Colloid Milium. -- This is seen in the South and Southwest in
sun-exposed fair-skinned individuals and is more or less irreversible.
Suggestions or comments for the editor:
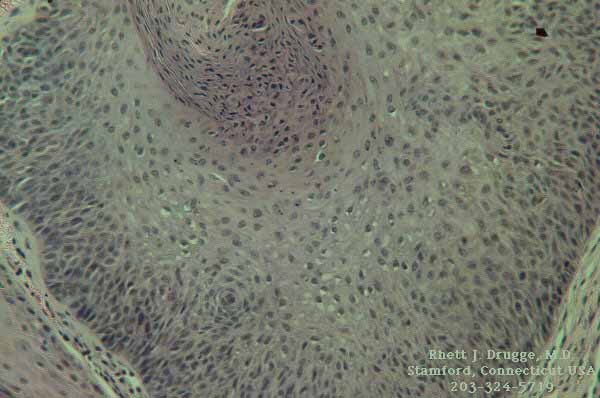
Actinic Keratosis
Actinic
Keratosis , LM
. -- Five percent 5-FU in hydrophilic petrolatum, rubbed in
twice a day for 3 to 4 weeks, or 1% 5-FU in propylene glycol is
an effective way of controlling these things. It does a wonderful
job, but the irritation response has to be watched closely. Roche
has a commercial preparation (Efudex). If it is used on lip keratosis,
where it is equally effective, prepare your patient for a horrendous
reaction.
Seborrheic dermatitis and sun exposure coincidentally produce
intensification of the response so that seasonal limitations are
wise. Bowen's disease of the face does respond to treatment, (LM)
although the condition of tone patient with hand involvement failed
to clear completely after many months of treatment. The duration
of treatment on the hands and forearms should be at least 6 week;
it is worthy of trial in treating erythroplasia of Queyrat or
extramammary paget's disease (case
report ). The iceberg effect of ending up with a more extensive
response than expected should be explained ahead of time. The
propylene glycol tends to dry the area, so bland emollients or
steroid and emollient for nightly use are helpful. Lotion makeup
to cover in the daytime helps women. Liquid nitrogen applied for
15-25 seconds is pleasanter and faster. If 0.5% triamcinolone
acetonide is used with the fluorouracil, the inflammatory reaction
is considerably lessened and the therapeutic result is the same.(ref
) On occasion telangiectasia may be an annoying side effect
of this combination, however. Better to avoid the fluorinated
steroids here and use plain hydrocortisone emollients.
Genetic Radiosensitivity
Xeroderma Pigmentosum. Clinical (1
, 2
, 3
, 4
, 5
, 6
) This disease is marked by accelerated actinic damage leading
to early metastatic disease. It can be helped with 5-FU treatment
and sun avoidance. Poikilodermatous changes presage the development
of skin cancer (keratoacanthomas, basal cell (LM),
squamous cell and malignant melanoma (OMIM
, (2
)).
Cockayne's Syndrome. --The key features of this autosomal recessive
disease are features of dwarfism and mental retardation, sun sensitivity(OMIM
).
DeSanctis-Cacchione syndrome-cutaneous photosensitivity and central
nervous system dysfunction are the key findings.
Bloom's Syndrome. -- Bloom syndrome is an autosomal recessive
disorder characterized by proportionate pre- and postnatal growth
deficiency; sun-sensitive skin (leading to poikiloderma); predisposition
to malignancy; and chromosomal instability. Diabetes mellitus
of insulin resistance, developing in the second or third decade
is a frequent feature (OMIM
).
PIBI(D)S. photosensitivity (P), ichthyosis (I), brittle hair
(B),impaired intelligence (I), possibly decreased fertility (D),
and short stature (S) (OMIM
)
Nevoid Basal Cell Carcinoma Syndrome (Gorlin's Syndrome), (patient
advocacy ) The most frequent findings in this autosomal dominant
condition are multiple basal cell carcinoma and odontogenic jaw
cyst. A substantial proportion (40%) are new mutations (OMIM
).
Erythropoietic Porphyria.
Hepatic Porphyrias. -- There are two types: the acute intermittent
and the cutanea tarda, clinical (1
, 2
) . The latter is more commonly seen, producing photosensitivity
in the exposed areas, e.g., bullae on the dorsa of the hands,
showing pink urine with the Wood's lamp examination. This condition
usually is seen in liver damage from barbiturates, contraceptive
pills, estrogens, alcohol or diabetes. The treatment is phlebotomy.
Acquired Radiosensitivity
Pellagra. -- Pellagra is classically seen in the elderly recluse
with poor nutrition and too much alcohol intake. Treatment is
nicotinic acid.
Systemic Lupus Erythematosus. -- Antinuclear
antibodies and a positive lupus
band test , hematuria, leukopenia and the malar
flush in a sick patient with oral
ulceration require steroids and antimalarials in combination
plus other tender loving care. Periungual
telangiectasia may ulcerate. Histopathologic criteria include,
epidermal atrophy, follicular hyperkeratosis, thickened basement
membrane, vacuolar interface dermatitis, pigmentary incontinence
and perivascular mononuclear inflammation. Subacute lupus features
identical laboratory findings associated with a light sensitive,
polycyclic
marginal erythema .
Discoid Lupus Erythematosus. -- Discoid lupus erythematosus consists
of a persistent localized erythema, usually on the face (1
, 2
, 3
) and with a special predilection for the ears (1
, 2
) but can occur on the extremities and scalp (1
), often with adherent scales, patulous follicles with keratin
plugs, and usually followed by atrophy. The cause is unknown,
but the condition is aggravated or induced by sun. Butterfly lesions
are typical (1).
Spontaneous cure occurs, often without scars. However,
in the scalp the patches usually leave scars that destroy the
hair and look like pseudopelade. The erythrocyte sedimentation
rate is usually elevated, and there may be leukopenia.
Treatment
Local Treatment. -- Steroid aerosol spray given three times a
day and then gradually less often; fluorinated cortisone ointment
with or without occlusion are partially and often wholly effective
in clearing the lesion. Intracutaneous triamcinolone acetonide
injection may lead to rapid and lasting control, although monthly
retreatment is often necessary. Avoiding the sun with opaque blocks
is essential.
Internal Treatment. -- The antimalarials, introduced after World
War II, have markedly suppressive effects. Atabrine, 100 mg tablets,
stain the skin yellow. Aralen (Chloroquine), 250-mg tablets, Plaquenil,
200-mg tablets, and Camoquin, are varieties. The most effective
treatment is a combination of Chloroquine 65 mg, Atabrine 25 mg,
and Plaquenil 50 mg, called Triquin. Dosage varies from six to
one daily, usually three times a day initially, dropping to as
low a maintenance dose as can be found later. The major side effects
of irreversible retinopathy somewhat discourages its free use,
although there is probably a dose relationship; if small doses
are used for a short time, no great risk is seen. Opacities in
the cornea appear to be reversible when the antimalarials are
stopped, and other side effects such as nausea, diarrhea, drug
rash (often like lichen planus), lightening of the hair and aplastic
anemia have to be taken into account.
Other methods of treatment include gold sodium thiosulfate given
intravenously starting at 5 mg and increasing to 50 mg weekly
for 6-10 weeks.
Histopathologic changes are roughly the same for all forms of
lupus erythematosus.
There are essentially five kinds of pigmented nevi: (1) the
epidermal nevus or lentigo, (2) the junctional nevus at the
epidermodermal junction, (3) the dermal nevus in the dermis,
(4) the compound nevus, with dermal and junctional elements,
with or without hair, and (5) the blue nevus, which is made
up of spindle-shaped nevomelanocytes deep in the dermis and
which is usually of such a distinct slate-like color that diagnosis
is easy.
There is arguably a sixth type of pigmented mole, the protuberant
polypoid papilloma, which is usually flaccid with a narrow stalk
and most often located in the axilla and groin. Often actually
a fibroma, this occasionally contains nevus cells and so should
be classified with the moles. "Clip and blip" is the proper
removal technique.
The decision as to which moles should be excised completely,
which should be removed with a superficial cosmetically acceptable
result, which should be left alone and which should have a small
excisional biopsy can be made by physicians only after many
years of experience looking at moles and their microscopic tissue.
In general, when in doubt, perform a biopsy. If the patient
is concerned and if he or she is having any symptoms
from a mole, the tissue must be examined microscopically. Trust
your clinical judgment; in general it is reliable.
From the therapeutic viewpoint, the pigmented moles that are
subject to irritation by friction of clothing, or in other ways,
can degenerate and become malignant or at least mimic malignancy
sufficiently to cloud clinical judgment. These should be removed.
Junctional
Nevi , These can arise at birth or later; pigmented
nevi located on the genitals, palms and soles are usually
junctional nevi. If the nevus is smooth, hairless, flat
or only slightly raised and light to dark brown, with a
"superficial" look to it, it is probably a junctional nevus.
Bathing-Trunk Nevi. -- In large hairy moles that have
extensive dark pigment with a blackish tint, the danger
of the patient experiencing malignant degeneration even
before puberty is great. Excision and flap or graft is the
method of choice. Andrews has used cryotherapy successfully
for inoperable cases.(ref. )
Mongolian Spot. -- This is a blue nevus over the sacrum
in dark-skinned newborns. It usually fades.
Spitz Nevi. --
C. The Significance & Importance of Dysplastic (Atypical
Nevi)
Lower Lip (1)
, (2)
, LM
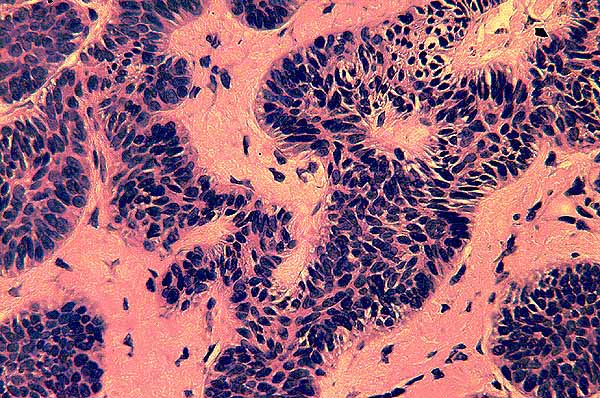
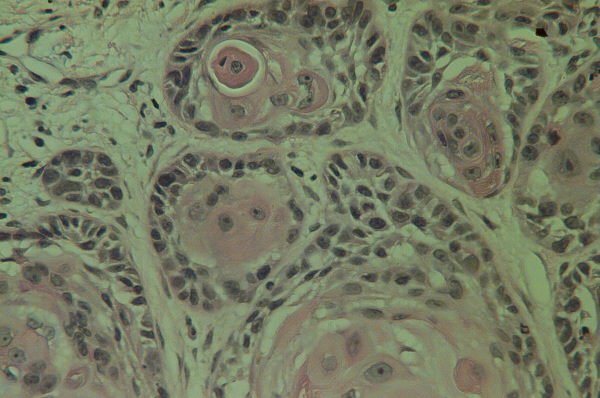
Oral SCC (1)
(LM, well-differentiated, keratinizing
pearls). SCC pr
On the glabrous skin this presents as a warty fast-growing nodule,
usually on the hand, lip,
ear or face. This carcinoma has a base that is usually indurated
and rounded and may be dusky red or purple. Crusted ulcerations
may occur. If left untreated, metastases will occur sooner from
tumors at the mucocutaneous junctions. Anaplasia can be severe,
especially at sites of radiodermatitis, and rapid removal is imperative.
Suggestions or comments for the editor:
Screening for malignant melanoma is imperative as the only cure
is early detection and removal. The metastatic potential of a
melanoma is directly related to it's depth of penetration (Breslow
depth). The warning signs of early melanoma are A, asymmetry,
B, border irregularity, C, colors, two or more, and D, diameter
greater than 6 mm, the approximate size of a pencil eraser.
6 key risk factors influence risk of developing malignant
melanoma:(Adopted from Darrell S. Rigel, M.D.)
1. Red/blond hair
2. Family history of malignant melanoma
3. Actinic keratoses
4. Marked freckling of upper back
5. 3 or more blistering sunburns prior to age 20
6. 3 or more years of an outdoor teenage summer job
With the above model, lifetime risk of malignant melanoma is:
1% with no factors
3-4% with 2 factors
20-25% with 3 or more factors
Lentigo
Maligna , Hutchinson's malignant freckle is usually a slowly
enlarging dark brown or black freckle on the cheek of an elderly
patient, which microscopically is malignant melanoma, but which
clinically runs an essentially benign course for years (up to
25) until eventually invasive malignant melanoma supervenes. It
can be cured by complete though superficial removal by any satisfactory
method, including electrodesiccation. It occasionally occurs in
the scalp, where it may infiltrate and pigment canities (case
report).
Acral Lentiginous Melanoma. -- Such a melanoma should be biopsied
and diagnosed early, since cure by amputation of the digit yields
a favorable outcome in most cases. Sometimes in a subungual position
it is mistaken for a fungus infection. It usually starts as alight
brown spot on the lateral nail fold or a vertical brown streak
running the length of the nail. When such a change is noted, a
nail fold or matrix biopsy is indicated.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}